The Texas Shooter and Involuntary Commitment
In 1995, Connecticut Governor John Rowland signed a bill to close Norwich and Fairfield Hills Hospitals, two of the state’s three public mental institutions. The hospitals had collectively housed more than 9,000 patients at their peak in the middle of the 20th century. By 1995, fewer than 700 patients remained.
Each of the three hospitals were state-run and staffed by unionized public employees. The hospital campuses were built before the second World War, and their aging physical plants required significant upkeep to satisfy federal regulators. It cost the state more than $100,000 per patient per year to operate the facilities, and officials estimated that consolidating public inpatient services to the state hospital in Middletown would save the state $13.7 million.
Connecticut, like most states, was winding down its inpatient population. State and federal law had made it more difficult to commit someone who was not imminently dangerous to himself or others to an inpatient facility. By 1995, the average patient who remained at the hospitals was generally sicker and more expensive to treat than the average patient had been 40 years prior. By the time Rowland announced the closures, no one in Connecticut was being institutionalized for “hysteria” or “burnout.”
Civil-rights litigators also pressured the state to reduce its institutional population. In 1990, a group of non-profits brought a class-action lawsuit against the state on behalf of people with traumatic brain injuries and intellectual disabilities in each of the three state hospitals. Attorneys for the plaintiffs argued their clients were placed in inappropriately restrictive settings in violation of federal law. They kept the class-action suit going for more than four years. By the time the case was settled, Connecticut had already announced it was closing the hospitals in Preston and Newtown.
In the decades since two of its three mental hospitals closed, Connecticut, like most states, has suffered an acute shortage of psychiatric beds. The statewide inpatient-utilization rate, which measures the number of psychiatric patients treated in inpatient settings versus the number of beds allocated by the state and private providers, is upwards of 120 percent. In other words, there were more psychiatric inpatients in Connecticut than there were beds allocated to treat them.
This presents several problems. For one, it forces suicidal, homicidal, and otherwise acutely ill patients to wait in emergency rooms for days or weeks on end for a vacant hospital bed. As of this writing, there are no vacant beds in the civil section of Connecticut’s large state hospital in Middletown. For another, it discourages people with acute conditions from coming forward to seek inpatient care in the first place. Finally, by effectively reserving the beds at the large state institutions for the most difficult cases—those immediately dangerous to themselves or others, and those with treatment-resistant psychosis—individuals with mental illness living in the community who need more intensive services than the community can provide are left to devolve until they become so ill that they either make an attempt on their own lives or, in rare cases, the lives of others.
You cannot draw a straight line between the closure of a hospital and an act of mass violence by a person with mental illness, but there is at least a chilling irony in the fact that an 18-year-old man with untreated serious mental illness killed 20 children at Sandy Hook Elementary School less than five miles from the grounds of the abandoned Fairfield Hills Hospital.
* * *
Texas’s mental-health system is, in certain ways, better than Connecticut’s.
Texas operates ten state hospitals and funds more than 2,200 public psychiatric beds. Its inpatient-utilization rate is less than 100 percent, reducing the chance that a psychiatric patient will be stranded in an emergency room.
State law also allows prosecutors and family members to initiate commitment proceedings when a person is unable to care for himself or is otherwise so disabled as to require hospital care, allowing families and communities to intervene before a person with serious mental illness deteriorates to the point of violence.
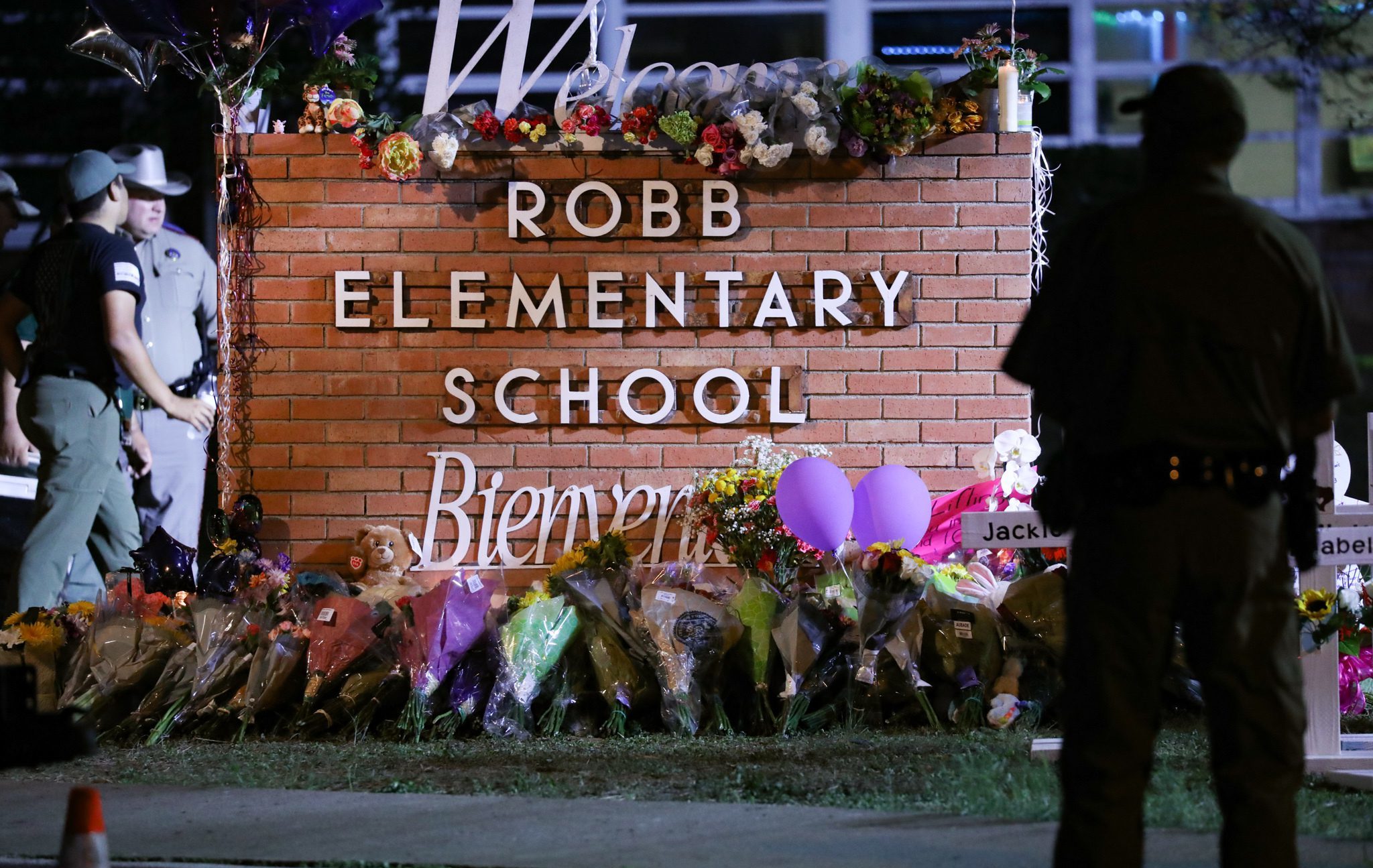
Yet the tragic events of Uvalde demonstrate that robust commitment laws and a well-funded network of state hospitals are of little use if the family and community surrounding a dangerous individual fail to intervene. And while it is unclear whether the shooter who killed 19 children in an elementary last week was “mentally ill”—he was never diagnosed as such and, unlike the Buffalo shooter, never confined for psychiatric treatment—his actions before the shooting suggest he should have been removed from his community regardless.
The Texas shooter reportedly tortured small animals and made regular threats against his classmates. His peers reported that he showed up to school with self-inflicted face wounds. In a sane society, that behavior would be grounds for intervention regardless of its clinical significance. A half-century ago, it would have landed him in a state hospital.
The shooter may have been sane. He may simply have been an evil person who did an evil thing. But whatever his behavior constituted under law—whether the threats he made were criminal in nature or the self-harm sufficient evidence to initiate a commitment hearing—it clearly merited intervention. It demanded a period of retreat, “asylum,” from his milieu.
That was, after all, the foundational purpose of the “insane asylum.” It is the reason that most state hospitals today are located in rural communities, with elegant buildings and bucolic grounds. The purpose of the “asylum” at its inception was to provide the mentally ill with a retreat from the wiles of urban life, a place to pray and reflect, be treated, and work out their neuroses and psychoses in pastoral quiet. Dr. Oliver Sacks, who worked with catatonic patients in New York and in several state hospitals across the country, said the asylum:
provided control and protection for patients, both from their own (perhaps suicidal or homicidal) impulses and from the ridicule, isolation, aggression, or abuse so often visited upon them in the outside world. Asylums offered a life with its own special protections and limitations, a simplified and narrowed life perhaps, but within this protective structure the freedom to be as mad as one liked and, for some patients at least, to live through their psychoses and emerge from their depths as saner and stabler people.
That the psychiatric institutions of the past were inadequate in serving this function does not mean that they could not be made adequate in the future.
Many state hospitals were often places of torment. There is a reason Connecticut closed two of its state hospitals. The civil libertarians who made it more difficult to commit a person to a mental facility were responding to real injustices in the mental-health system that should not be ignored.
Yet the words of one of Sacks’s patients are worth holding in mind: “Bronx State [Psychiatric Center] is no picnic, but it is infinitely better than starving, freezing on the streets, or being knifed on the Bowery.”
Committing a person like the Texas shooter, who may not have broken the law or been adjudged insane, to a state hospital may not suit our civil-libertarian sensibilities. But to use the words of Sacks’s patient, it strikes me as “infinitely better” than the alternative.



Comments